- Hypermobility and Exercise Part 2: Proprioception, Brain Maps and Why Your Body Feels Lost - 19 May 2026
- Hypermobility, EDS and Constipation: Why Your Gut Won’t Cooperate and What Actually Works - 18 May 2026
- Why Your Hypermobile Muscles Feel Tight and Weak at the Same Time: Understanding Muscle Tone - 14 May 2026
If you have hypermobility, you have probably noticed something about your feet. Maybe the arches look flat. Maybe they collapse inward the second you stand up. Maybe your ankles roll on uneven pavements, or your shoes wear down on the inside edge in a way that looks faintly criminal. You have probably also been told you overpronate, been handed a pair of orthotics, or been told to wear “supportive” shoes for the rest of your life. It isn’t a coincidence either: people with hypermobility consistently show reduced joint proprioception compared with controls in systematic review[15], and altered multisegment foot kinematics during walking[6].
And here is the bit nobody mentions. Foot and ankle problems don’t stay at the foot and ankle. They travel. Knee pain. Hip stiffness. SI joint nonsense. A whole lower body that feels like it’s working against you, when really it’s just been left to compensate for a foot that can’t do its job properly.
This blog is going to look at what the foot actually is, what tends to go wrong in hypermobility, and the work that genuinely changes things. We’ll cover the three points of contact, the build, collapse, rebuild cycle, the drive shaft at the shin bone, why orthotics don’t fix anything, why high arches are the other end of the same problem, why your brain is the limiting factor more often than your muscles are, and what we actually do in the studios to rebuild this from the ground up.
What this post does not cover: footwear reviews, specific orthotic brands, surgical opinions, or anything to do with kids. That’s all for another day.
So, if you’re ready to stop blaming the foot and start training it, let’s go.
Your foot is not a platform. It’s a sensory organ.
This is the reframe that has to happen first. Most people, and a lot of clinicians, treat the foot like a passive base. A thing that holds you up. A platform. The model is essentially “the foot supports you, so if it’s not supporting you well, we’ll add support”. Cue the insoles.
When it comes to sensory real estate, the sole of your foot is densely packed with mechanoreceptors. The same type of sensors that live in your fingertips. Direct microneurography recordings have mapped four distinct cutaneous receptor types across the human foot sole, each with their own firing pattern to indentation, stretch and movement of the skin[16]. They detect pressure, vibration, stretch, and changes in ground contact. They tell your brain whether you’re on a flat surface or an uneven one, whether your weight is shifting forward or back, and how fast force is arriving through the floor. That’s a lot of incoming traffic for something we tend to think of as just “the bit at the bottom”.
So the foot has two jobs. It absorbs and produces force, yes. But it also feeds the brain a constant, high resolution map of what is happening underneath you. And when the input is clear, the brain can make rapid, accurate decisions about how to activate the muscles, when to stiffen a joint, when to let it move, when to brace, when to soften. Walking becomes smooth and pretty much automatic.
When the input is fuzzy, the brain has to guess. And it doesn’t like guessing. It compensates. It braces. It co contracts. It locks joints. All of which increases effort and reduces efficiency, which is why a lot of those with hypermobility end up exhausted by 11am, and don’t quite know why. The proprioceptive deficit is the consistent finding in this population[15], and it shows up at the foot in both children[1] and adults[6].
Children with generalised joint hypermobility had reduced foot sole tactile sense and poorer ankle proprioception compared with peers [1]. Adults with hEDS and HSD walk with altered multisegment ankle and foot kinematics [6]. The foot is moving differently. Not because the person is doing something wrong, but because the information feeding the motor plan is unclear. The map is fuzzy, so the movement is fuzzy. Strength has very little to do with it.
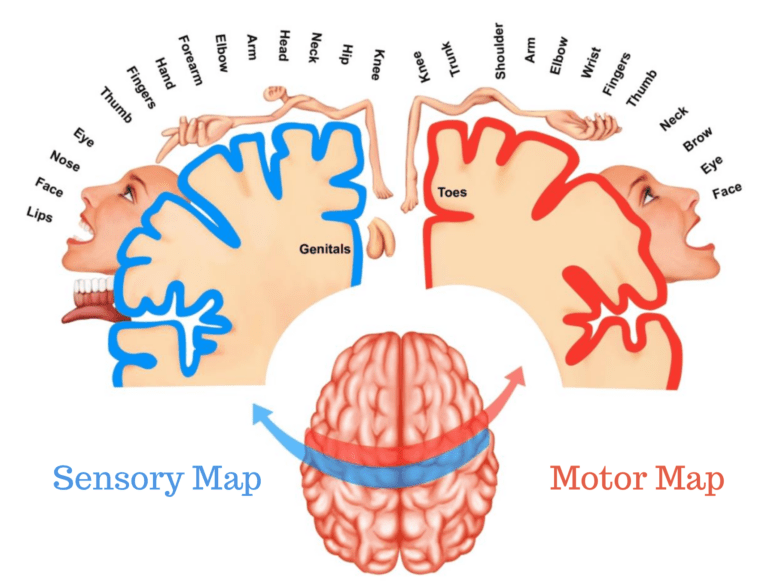
This is also why we’ve written elsewhere about cortical maps and proprioception at length. Before you can fix what the foot does, you have to fix what the brain knows about the foot. That bit isn’t optional.
The three points of contact
Everything starts here. Your foot is supposed to meet the ground in three places. The heel. The base of the big toe, that fatty pad on the inside of the forefoot. And the base of the little toe, the pad on the outside. Three points. Heel, point one (medial), point two (lateral). That’s it.
Together they form what’s often called the foot tripod. Three legged stool, basically. If all three legs are on the floor, the stool is stable. Remove one, or let one drift, and the whole thing wobbles. That stable base lets the muscles, ligaments and fascia of the foot work together. It also lets the receptors in those three pads send clear information up to the brain. Less stool, less signal.
For a lot of those with hypermobility, one or more of these contact points is inconsistent. The arch collapses so far inward that point one (under the big toe) lifts off, or the heel drifts. Or the outer edge of the foot ends up taking too much load because the brain is trying to brace against pronation. Either way, the tripod isn’t a tripod anymore. It’s a two legged stool and a wonky vibe. Adults with flat foot show altered kinetic and kinematic stability compared with healthy controls[8], and standing stability is reduced in flatfoot populations[9].
Awareness of these three points is where any genuine foot work begins. Not heel raises. Not arch lifts. Not “engage your core”. Where is the foot actually meeting the floor, and is it meeting the floor in the three places it’s supposed to. If not, that’s the first thing to sort. When it comes to the foot, no tripod means no foundation, and no foundation means everything above it gets harder than it should be.
A useful first cue: stand barefoot, feet hip width. Pull your toes up so you can’t grip the floor. Now, with the toes off the floor, feel for all three pads pressing down. Most people are missing point one. A few are missing point two. Some are mainly on the heel and barely on the forefoot at all. None of those are “wrong” in a moral sense. They’re just a map of where the work needs to start.
Build, collapse, rebuild: the cycle nobody talks about
When it comes to the foot conversation in the hypermobility world, it’s almost always one sided. The arches collapse, so we have to “lift” the arches. Done. Off you pop with your orthotic.
The problem is the foot isn’t supposed to hold an arch shape the whole time. It’s supposed to do the opposite. It’s supposed to build the arch, collapse the arch, and rebuild the arch. Every single step.
Here is what happens in a healthy gait cycle. You heel strike. The tibia (your shin bone) rotates internally, just a touch. The arch drops slightly. The foot softens, spreads, and absorbs the ground reaction force as it travels up through the tissue, the muscle, and the fascia. Then, as you push off, the tibia externally rotates. The arch rebuilds. The foot becomes a rigid lever for propulsion. And you move forward.
Build. Collapse. Rebuild. About a hundred and twenty times per minute when you walk at a normal pace. None of it under conscious control. Nobody is thinking “right, time to internally rotate my tibia” as they cross the road. This whole timing pattern is reliably disrupted at the foot in hEDS and HSD[6].
Now here is the bit that surprises a lot of people. The collapse is not a failure. It’s a feature. That controlled drop in the arch is how the foot absorbs landing forces. Without it, force just slams into the bones and goes looking for somewhere to dump itself.
Imagine you’re falling toward a door. If you put your arm out stiff and locked, all that force ploughs straight through the elbow and shoulder. Uncomfortable. Now imagine you fall toward the same door but soften everything. Bend the elbow, let the shoulder give. Same force, very different experience. The foot does the same thing. A foot that can collapse a little absorbs force smoothly. A foot that can’t, doesn’t.
And, equally, a foot that’s collapsed all the time and can never rebuild is also broken. Both halves of the cycle have to work. If you have high arches that are stuck up, you need to be able to collapse them deliberately. If you have flat feet that are stuck down, you need to be able to build them. Most people only train one half of that and then wonder why their feet still feel weird.
The drive shaft: why your shin bone is the real foot exercise
The tibia is basically a drive shaft sitting between the foot and the knee. When the shin bone rotates inward, it pulls the arch down through the joints below it. When it rotates back outward, it lifts the arch and re stiffens the foot for push off.
So when we say “the arch collapses and rebuilds with every step”, we’re really saying “the tibia rotates in and out with every step”. The arch is the visible part of a rotation that’s happening higher up. If you can control tibial rotation, you can control the arch. If you can’t, the arch is more or less stuck, and you’re left slamming the foot into the floor.
A small muscle behind the knee, the popliteus, is the muscle that initiates this. It unlocks the knee just before heel strike and lets the tibia rotate. The medial hamstrings, the semitendinosus and semimembranosus, also pitch in on the internal rotation side. None of these are muscles you have probably ever consciously trained. They tend to come back online as a side effect of doing the right work below them.
What we tend to see in hypermobility (this is clinical observation, not a hard study finding) is the opposite pattern. The biceps femoris, the outside hamstring, ends up overactive and effectively dominant. The medial hamstrings and the popliteus are quiet. The tibia ends up rotated in or out in a stuck position, with poor mid range control. The arch is pinned. The foot is pinned. The whole drive shaft is jammed. Sat alongside the measured kinematic differences in hEDS gait[6], that pattern explains a fair amount of the lower limb fallout we see.
The other thing we see, and it’s quite common, is what we call penguin feet. The femur is rotated inward, the tibia rotates outward to compensate, and the result is a foot that splays out to the sides and looks completely flat at rest. The arch has nowhere to go. Until you sort the rotation upstream, the foot will keep doing the same thing no matter how many short foot exercises you throw at it.
This is also why we wrote a separate piece on internal tibial rotation in detail. The foot work and the tibial rotation work are the same conversation. You can’t really do one well without the other.
Why orthotics aren’t the answer (most of the time)
When it comes to orthotics, this is the bit that tends to upset people, so let me be precise.
Orthotics are not the devil. They can offer temporary support. They can take load off a really irritated tissue while you do the work to change things. For some people, particularly during acute pain flare ups, they make a meaningful difference. We are not anti orthotic.
What orthotics don’t do is force adaptation. They don’t teach the muscles of the foot to work differently. They don’t sharpen the sensory map. They hold a shape that the foot can’t yet hold for itself, which is fine as a scaffold, but a scaffold is not a building. If the scaffold is the only thing keeping the structure up, you have a long, expensive future of replacing scaffolds.
Compare that with what happens when you actually train the foot. Short foot exercises, which train the arch from the inside out, were more effective than arch support insoles for improving the medial longitudinal arch and dynamic balance in adults with flexible flatfoot [4]. Training the small plantar intrinsic muscles improved both arch morphology and dynamic function [5]. Four weeks of short foot training beat towel curls for both static and dynamic balance tasks [7]. A 2024 meta-analysis pulled the literature together and concluded that short foot training improves foot posture in flatfeet [11], and a randomised controlled trial showed that adding short foot work to balance rehab improved outcomes in flat foot [10].
So the foot can change. The arch is not a fixed structure. The muscles can be retrained. The map can be sharpened. It just needs the right input.
There’s also the question of what’s actually wearing thin. Adults with flat foot showed altered kinetic and kinematic stability measures compared with healthy controls [8], and standing stability is genuinely affected by flatfoot mechanics [9]. So we know the consequences. We also know they aren’t permanent.
An orthotic might let you walk to the train station today, which is fine, occasionally necessary, and well worth it. It just shouldn’t be the whole plan.
High arches: the other end of the same problem
A quick word on this, because it gets ignored constantly. Half the foot conversation in the hypermobility space assumes everyone has flat feet. They don’t. Plenty of those with hypermobility have very high arches. The arch is stuck up rather than stuck down, and the standard advice (“strengthen the arch, do short foot exercises, wear arch support”) doesn’t just fail to help, it actively makes things worse.
Here’s the picture. If your arch is locked high, you’ve got the opposite of the flat foot problem. The foot can’t collapse. It can’t soften. It can’t absorb the ground reaction force, so every step is a small impact event that travels straight up the leg. People with high arches showed higher peak plantar pressures under the heel and forefoot and significantly more foot pain than people with neutral feet [12]. The pain wasn’t theoretical, it was measurable.
It also affects how far you can move the ankle. People with idiopathic high arches had significantly reduced weight bearing dorsiflexion compared with neutral and flat feet [13]. Translation: when you walk, your shin can’t travel as far forward over the foot, so you end up taking shorter steps without realising it. You compensate. The hip works harder. The Achilles and calf complex stays under constant tension. The plantar tissue at the bottom of the foot ends up pulling on attachments it shouldn’t be pulling on. This is also why different arch types end up with different injury patterns in active populations [14], and why a runner with high arches and a runner with flat arches need almost opposite interventions.
For those with hypermobility, this gets worse, not better, than it does for the general population. Joints that should mechanically stop a movement don’t, because the tissue is more lax. So the foot can’t dorsiflex, but the body finds a way around it by pulling through tissues that were never designed to be the brake. Plantar fascia. Achilles. Calves. People with very high arches and hypermobility tend to collect the full set: plantar pain (which usually gets labelled plantar fasciitis, although technically it’s more like a tendinopathy of the same tissue), tight calves, irritated Achilles, sometimes arthritis in the big toe joint because the joint above it has been compressed for years. None of that is bad luck. It’s a stuck up arch doing what a stuck up arch does.
Here’s the part that catches people out. The work for high arches looks superficially similar to the work for flat feet. Three points of contact. Tibial rotation. Build, collapse, rebuild. Slow, attentive reps. But the focus is the opposite. With flat feet you spend most of your effort training the build. With high arches you spend most of your effort training the controlled collapse. The arch needs to come down, on demand, smoothly, without crashing through to the floor and without locking up halfway. You’re teaching the foot to soften.
The cross foot stabilisation cue also flips. Flat footed people usually need to be reminded to keep point one (the big toe pad) pressing into the floor, because they’re rolling inward and that point is lifting off. High arched people are the opposite. They tend to roll out, and point two (the little toe pad) is the one that lifts. So the tactile band, the cue we use in the studios for sensory feedback, goes under point two instead of point one. Same cue. Different foot. Different reminder.
A very common scene, by the way: someone with high arches who has been told for years their arches “never touch the ground”, who has been wearing rigid orthotics that hold the arch up even further, and who has slowly developed pain in the big toe, the Achilles, and the lower back. The orthotic was solving the wrong problem. It was holding the arch in the position it was already stuck in. The work is to teach the foot to come down, not to be held up.
So if you’ve read everything above and thought “none of this applies to me, my arches are too high”, I’d push back. It applies more, not less.
Sensory orthotics, taping, and the difference between propping and informing
When it comes to what you put in your shoes, one important distinction matters.
There’s a useful split here. There are two very different types of “thing in your shoe”. There are supportive orthotics, the rigid ones designed to hold the foot in a particular position. And then there are sensory orthotics, the textured ones, sometimes a piece of foam with bumps on, sometimes a piece of tape on the skin. They feel almost insignificant by comparison.
The sensory ones work in a completely different way. They aren’t holding the foot up. They’re talking to it.
Somatosensory orthoses improved postural control in people with hEDS in a pilot study [3]. A case report on neuromuscular taping in a person with joint hypermobility syndrome/Ehlers-Danlos showed improved ankle position at initial contact during walking [2]. That’s a single case, so we can’t draw broad conclusions from it. But it’s consistent with the same principle: enhanced sensory input changes motor output. When the brain gets clearer information about what the foot is doing, it makes better decisions about how to use it.
Which is why a textured insole the thickness of a credit card can sometimes do more for someone with hypermobility than a moulded carbon fibre orthotic. The textured one is feeding the brain. The moulded one is just holding the foot.
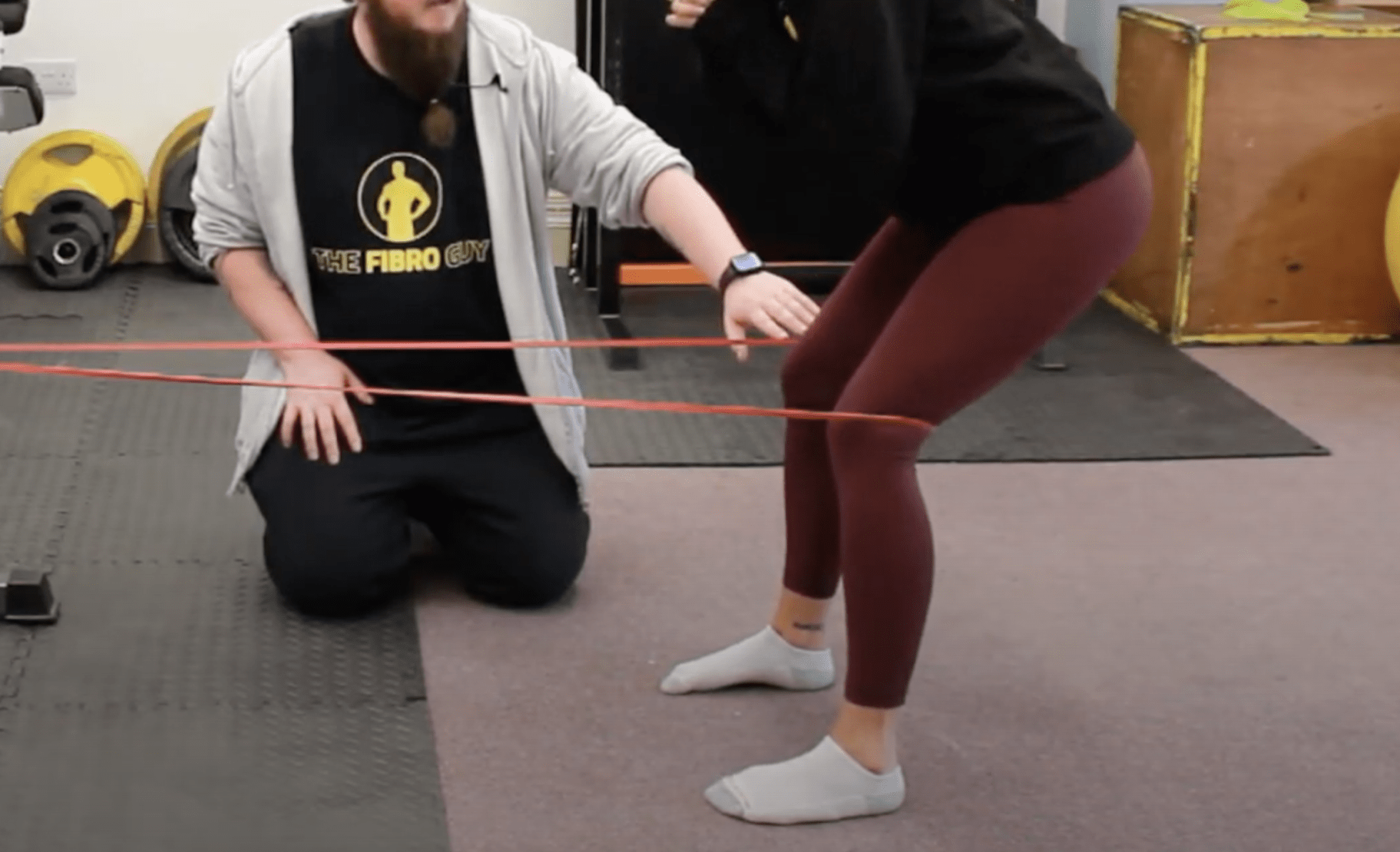
It also explains the cue we use a lot in the studios: place a light band around the foot or ankle during a drill. It’s not for resistance, the band is way too light to do anything mechanically. It’s there as a tactile cue. The skin pressure under the band tells the brain “your foot is here”. Once the map is clearer, the foot moves better. Then, eventually, you take the band off and the movement holds because the map was the thing that was missing in the first place.
The 4mm shoe sole rule
When it comes to shoes, this isn’t research, it’s a rule of thumb we’ve used in the studios for years. Anything over about 4mm of sole between your foot and the floor starts to noticeably impact proprioception. You can’t feel what you’re standing on, so the brain has less information to work with.
It doesn’t make thick soled shoes evil. Sometimes you genuinely want a chunky sole for a long day on concrete, or for sport. But for general daily wear, especially when you’re trying to rebuild the foot, the thinner the sole, the better the signal. Sole thickness matters more than brand. In a classic balance study, thicker and softer shoe soles reduced standing balance compared with thinner harder soles, the opposite of what you’d expect if cushioning helped[17]. A flat, thin soled trainer beats most “supportive” running shoes for everyday use during the rebuilding phase.
This doesn’t mean go barefoot everywhere. Barefoot on tarmac at 8am in February isn’t the answer either. It just means know what your shoe is doing. A 30mm stack with a “stability post” is essentially turning the lights down on your foot’s relationship with the ground, which is exactly the input the receptor mapping work shows the brain depends on for postural control[16]. Which might be exactly what you want for one specific situation, and exactly what you don’t want for the other twenty hours of the day.
What “control” actually looks like in practice
Right, theory’s lovely. What does this look like when you’re actually doing the work? The video below shows the core arch control pattern we teach. Watch it once, then come back for the breakdown.
So, what’s going on there. A few things.
First, the three points of contact. The big rule is all three points stay on the floor the whole time. The classic mistake is to push the weight to the inside of the heel and let point two (the little toe pad) lift off the floor. The other classic mistake is to push to the outside of the heel and let point one (the big toe pad) lift off. Either way, you’ve made the foot a two legged stool. Keep all three down. If a point lifts, that’s your cue you’ve gone too far.
Second, the cross foot stability cue. Weight shifts slightly to the outside of the heel, and as it does, gently press down through point one (the big toe pad). That tiny opposing pressure is what keeps the foot crossed and stable. It feels weird to start with because most people with hypermobility have either lost point one entirely, or they’re hammering it because the foot has rolled inward, and the idea of pushing it down deliberately while the heel is on the outside feels backwards. It isn’t.
Third, the toes. Start with the toes lifted. That cuts out the long flexors that try to grip the floor and “fake” the arch. With the toes up, you can’t grip. You have to use the actual foot. Once the pattern is in, you can lower the toes and the arch should stay up by itself. This is also where the classic doming mistake comes in. People grip the toes, the toes shorten the foot, point one lifts off the floor, and the whole tripod collapses. If the toes are gripping, you’re cheating.
Fourth, the speed. Slow. Painfully slow at first. We have a thing we say in the workshops: speed hides need. If you go fast, the system will brace, lock everything down, and “pass” the drill on momentum and stiffness. You will feel like you did it, but the foot will have learned nothing. Slow it right down and a lot of people discover that the arch flickers. It oscillates up and down without control because the muscles can’t grade it yet. Flickering is normal at the start. It tells you exactly where the control isn’t, which is honestly the most useful thing you can find out.
Fifth, and this is the unglamorous one, breathing. A surprising amount of people hold their breath when they do this. The minute the breath goes, the body locks down, sympathetic tone goes up, and the foot stops being able to feel anything. If you notice your shoulders rising, your jaw setting, or your breath disappearing, you are gripping the rickety bridge. Drop the bridge. Breathe out. Try again.
The tibialis anterior arch lock
One muscle worth singling out. The tibialis anterior. It runs down the front of your shin, attaches under the arch, and when it contracts it pulls the foot into dorsiflexion (toes up) with a bit of inversion (rolling outward). Translation: the TA can lift and lock the arch.
For a lot of those with hypermobility, the TA is sleepy. It’s there, it’s anatomically intact, but it doesn’t fire when you’d expect it to. So we have to wake it up deliberately. We use it as an active locking mechanism for the arch on one leg work, balance work, and any time we want the foot to be steady under load.
Practical version. Stand on one leg. Three points down. Now actively pull your foot up and slightly inward without rolling the ankle over. You should feel the TA fire down the front of your shin. It will feel a bit intense the first time. Some people can’t do it at all without the other leg flailing for balance, which is fine, you’ll get there. You can co contract the calf at the same time to lock the ankle from both sides. The arch ends up high and rigid, the foot becomes a stable platform, and the work above the foot (knee, hip, trunk) suddenly gets easier because it isn’t fighting a wobbly foundation.
Where this falls apart is when the tibia and femur start rotating as one block. The foot wants to rotate inward, but the whole leg comes with it. A band cue on the outside of the knee, pulling for external rotation, frees up the foot and lets you find the TA without dragging the whole leg into the movement. We use that one a lot.
Variation is the point, not the enemy
When it comes to foot rehab as it’s usually taught, the obsession is always with reps. “Do this short foot exercise three times a day for 10 reps.” And then nothing changes, because the foot has learned exactly one thing: how to do one specific movement, in one specific position, on one specific surface.
Real walking doesn’t look like that. Real walking is fast, slow, uphill, downhill, on grass, on tile, on a kerb you didn’t quite see. The brain needs to have practiced the pattern in lots of conditions, otherwise it won’t transfer.
So once you can do the basic arch lock, you start changing things. Slow it down. Speed it up. Do half a rep. Hold the top for a second. Hold the bottom for a second. Add a metronome at 60 BPM, then at 90. Close your eyes. Stand on a thin mat. Stand on a thicker mat. Do it standing, then sitting, then in a half kneel. Every change forces the brain to rebuild the pattern slightly, which is exactly what we want.
There’s a piano analogy that might help. If you learn one tune perfectly, you can play that tune. If you learn lots of tunes badly first and then get better, you become a piano player. The brain learns the underlying skill, not the specific tune. Foot work is the same. Lots of variation, played badly to start with, beats one perfect rep done a thousand times.
And honestly, the things that ruin foot work the fastest are: doing the reps too fast, gripping the toes, holding the breath, and chasing numbers. None of those are about the foot. All of them are about how a hypermobile nervous system tends to default to “brace” when it isn’t sure. Less brace, more attention, slower reps, fewer numbers. That’s the recipe.
A word on shoes, mats, and the surfaces you actually live on
You can’t only train the foot in your living room and expect it to suddenly work on a wet pavement. The cortical map you build is partly tied to the surfaces you build it on. Carpet only is fine for a few weeks while you get the basics, but after that the foot wants variety.
Textured mats are useful for proprioceptive training, because the surface itself feeds the foot a different signal every time you shift weight. The skin gets stretched in tiny different ways, and the brain has to update its map continuously. That’s exactly the kind of input that thickens the sensory representation of the foot in the brain.
Walking barefoot at home, if your floors aren’t freezing, helps for the same reason. Stones, sand, grass, all of it, the brain loves new textures. Whereas walking around in chunky soled trainers all day with 30mm of foam between you and the world is the opposite. The foam smooths out the signal. Your brain ends up with the same fuzzy input it would get if you’d put a glove on your hand and tried to read braille.
So mix it up. Different shoes for different situations. Different surfaces during practice. Different speeds. Different focus points. The foot is asking for variety, and most of us have spent decades giving it the same flat floor at home, the same office chair, and the same supportive shoe for the school run.
When you put it all together: the way walking is supposed to work
So, what does a sorted version of all this actually look like? Let’s run a single step in slow motion.
Your back foot is about to swing through. The popliteus on the front leg fires just before heel strike, unlocking the knee. As the heel hits the floor, the tibia rotates internally. The medial hamstrings help. The arch drops slightly. The forefoot rolls through, points one and two find the floor, the load spreads across the tripod. The tibia then begins to externally rotate. The biceps femoris and other lateral structures come in. The arch rebuilds. The foot becomes rigid. You push off through points one and two. The back leg swings, and the cycle repeats on the other side.
Build, collapse, rebuild. About a hundred and twenty times a minute, in time, on time, automatically, without you having to think about it.
What we tend to see in hypermobility is some version of: the popliteus is asleep, the tibia is stuck either rotated in or rotated out, the medial hamstrings are quiet, the biceps femoris is doing everything, the arch never properly drops because it’s already at the floor, or it never properly builds because nothing tells it to. The foot strikes hard. The force rebounds and travels up the leg. Wherever the weak link sits, that’s where the force concentrates. Sometimes the ankle. Sometimes the knee. Often the SI joint. Sometimes the lower back. People then go and have the painful joint treated, when really the painful joint is the symptom and the foot is the cause.
This is why we so often have to work backwards. Pain at the SI? Have a look at the foot. Knee pain on one side and not the other? Have a look at the foot on that side. Hip that locks up after walking? Have a look at the foot. Not always, but a lot of the time, the answer is upstream of where the pain is, in the joint that nobody has ever properly trained.
Why “just strengthen the foot” usually fails
You will see a lot of well meaning advice online that boils down to: “your arches are weak, do these three exercises every day, and they will come back”. And it isn’t wrong, it’s just incomplete enough to mostly not work.
Strength is rarely the bottleneck in hypermobility. The map is. The timing is. The sensory feedback is. The proprioception evidence is consistent on this point[15]. You can do all the toe scrunches in the world and not change the fact that the brain doesn’t trust the foot enough to switch the right muscles on at the right moment. The arch may collapse not because the muscles can’t lift it, but because the brain isn’t confident enough to activate them when it needs them.
This is the bit where the cortical map work and the foot work meet. You can’t really separate them, even though they get taught separately. If the map is fuzzy, no amount of strength fixes the timing. If the timing is on, the strength tends to come along for the ride, because the muscles are finally being used the way they’re built to be used. Most of the people we work with don’t need more strength. They need a clearer signal.
Now, this doesn’t mean strength is useless. It just means it’s downstream of sensory clarity. First the map, then the tone, then the strength. Get the order right, and the work goes faster. Get the order wrong, and you end up frustrated, hammering tissue that doesn’t know what it’s supposed to do yet.
The bigger picture: what we’re really training
What you’re really training isn’t the foot. It’s the conversation between the foot and the brain. The map gets clearer. The cycle gets smoother. The muscles get used the way they’re built to be used. The brain stops bracing and starts grading. The bracing comes down. The tone comes down. Walking stops being exhausting.
That’s the goal. Not a “good arch” in some textbook sense. Not perfect biomechanics. Just steadier, more controlled, more efficient. A foot that does its job without you having to think about it. A nervous system that has enough information to relax. The proprioceptive deficit in hypermobility is consistent across studies[15], which means it’s a target the work can actually move.
And the encouraging bit is that all of this is trainable. The maps can sharpen. The timing can improve. The literature on short foot training, intrinsic muscle work, and sensory focused rehab consistently shows improvements in arch morphology, balance, and motor control [4][5][7][10][11]. It isn’t quick, and it isn’t linear, but it’s reliable, given enough consistent practice. Bodies adapt. Brains rewire. Feet rebuild.
Common mistakes we see in the studios
To save you a few months of trial and error, here are the patterns we see most often. None of them are dealbreakers. All of them are fixable. They’re worth keeping in the back of your head when you’re practising.
Gripping the toes. The single most common one. The long flexors fire, the toes curl into the floor, and point one lifts. The arch goes up, but only because the foot has shortened, not because the intrinsics have done anything. Lift the toes. Try again.
Rolling onto the outside edge. Sometimes people massively overshoot the “weight to the outside of the heel” cue and end up balanced on the lateral edge of the foot, with point one lifted off entirely. The foot looks vaguely like a banana. That isn’t cross foot stabilisation. That’s just rolled out.
Doing it on autopilot. Banging out 30 reps while watching TV is genuinely a waste. The foot needs your attention. Twenty good slow reps with full attention beats two hundred mindless ones. We’ll go over this in part one of the exercise series in a bit more depth.
Chasing numbers too early. “How many sets, how many reps” is the wrong question for the first few weeks. The right question is “can I do this slowly without flickering, without holding my breath, and without my knee swinging in or out”. Once that’s solid, then we add load and reps. Not before.
Letting the knee drop in or kick out. Particularly common during one leg work. The foot tries to do its job, the knee starts wandering because the hip isn’t holding well, and the foot ends up either flat or rolled out depending on which way the knee went. A band cue at the knee is useful here. We tend to use a light band for tactile feedback, not for resistance.
Practising one foot at a time and then walking on both. This sounds obvious, but practising one side, switching to the other, and never combining is a habit a lot of people fall into. The drills are unilateral. Walking isn’t. Once the basics are in, we want bilateral work, two leg drills, then walking drills, then real walking. Otherwise you build a beautiful arch that only works while you’re standing on one leg in the kitchen.
A note on timeline (no, it isn’t going to fix itself in two weeks)
When it comes to timeline, this is the bit that nobody wants to read but everybody needs to. The map work, the timing work, the rebuilding of foot control, isn’t quick. The first three to five weeks are mostly invisible, in the sense that on the outside it looks like nothing is happening. Your arch isn’t suddenly higher. Your gait isn’t visibly different. Most of the change is neural, and neural change is silent for a while.
What tends to show up first isn’t the arch lifting. It’s small things. You suddenly notice your foot during a walk. The wobble at one specific point in the stride. The fact that one side feels heavier than the other. A flicker that’s there one day and gone the next. The brain is paying attention to the foot in a way it wasn’t before. That’s the change. The visible bit comes later.
So if you do four weeks of this and your arches still look the same in photos, you’re doing fine. Keep going. The bit you can see is the last bit to change.
Where to go next
If you’ve made it this far, you have probably figured out that arch work isn’t really about the arch. It’s about cleaning up the input to a foot the brain has stopped paying attention to. The drills, the cues, the bands, the textures, the slow tempo, all of it is feeding the foot back into the brain’s awareness. Once that’s done, the arch tends to sort itself out, because the foot finally has the information it needs to do its actual job.
If you want a structured, progressive version of all of this, with proper follow along sessions, the drills, the variations, and the integration into walking, we’ve built a dedicated course for it. It’s called Building Your Foot Arch, and it’s the same framework we use in the studios. Five progressive blocks, short talks plus practical drills, minimal equipment, lifetime access. It runs through everything in this post and a lot more, plus the dynamic work that’s hard to describe in writing.

And if you want to dig further into the bigger picture, the cortical map work that sits underneath everything we do is covered in our piece on cortical maps and proprioception, and the tibial rotation drills that pair with the foot work are in our piece on internal tibial rotation. They’re both worth a read if you want the full set of moving parts.
The foot is the bit underneath everything. When it stops doing its job, everything above it works harder than it needs to. When it starts doing its job again, a lot of those upstream problems quietly resolve themselves. It’s slow, unglamorous, and almost embarrassingly simple in places. It also works.
References
[1] Akkaya KU, Burak M, Yildiz R, Yildiz A, Elbasan B. Examination of foot sensations in children with generalized joint hypermobility. Early Human Development. 2023;180:105755. doi: 10.1016/j.earlhumdev.2023.105755
[2] Camerota F, Galli M, Cimolin V, Celletti C, Ancillao A, Blow D, Albertini G. The effects of neuromuscular taping on gait walking strategy in a patient with joint hypermobility syndrome/Ehlers-Danlos syndrome hypermobility type. Therapeutic Advances in Musculoskeletal Disease. 2015;7(1):3-10. doi: 10.1177/1759720X14564561
[3] Dupuy EG, Leconte P, Vlamynck E, Sultan A, Chesneau C, Denise P, Besnard S, Bienvenu B, Decker LM. Ehlers-Danlos Syndrome, Hypermobility Type: Impact of Somatosensory Orthoses on Postural Control (A Pilot Study). Frontiers in Human Neuroscience. 2017;11:283. doi: 10.3389/fnhum.2017.00283
[4] Kim EK, Kim JS. The effects of short foot exercises and arch support insoles on improvement in the medial longitudinal arch and dynamic balance of flexible flatfoot patients. Journal of Physical Therapy Science. 2016;28(11):3136-3139. doi: 10.1589/jpts.28.3136
[5] Mulligan EP, Cook PG. Effect of plantar intrinsic muscle training on medial longitudinal arch morphology and dynamic function. Manual Therapy. 2013;18(5):425-430. doi: 10.1016/j.math.2013.02.007
[6] Vermeulen S, De Mits S, De Ridder R, Calders P, De Schepper J, Malfait F, Rombaut L. Altered multisegment ankle and foot kinematics during gait in patients with hypermobile Ehlers-Danlos syndrome/hypermobility spectrum disorder: a case-control study. Arthritis Care and Research. 2022;74(5):841-848. doi: 10.1002/acr.24526
[7] Lynn SK, Padilla RA, Tsang KK. Differences in static- and dynamic-balance task performance after 4 weeks of intrinsic-foot-muscle training: the short-foot exercise versus the towel-curl exercise. Journal of Sport Rehabilitation. 2012;21(4):327-333. doi: 10.1123/jsr.21.4.327
[8] Sung PS, Zipple JT, Andraka JM, Danial P. The kinetic and kinematic stability measures in healthy adult subjects with and without flat foot. The Foot. 2017;30:21-26. doi: 10.1016/j.foot.2017.01.010
[9] Tahmasebi R, Karimi MT, Satvati B, Fatoye F. Evaluation of standing stability in individuals with flatfeet. Foot and Ankle Specialist. 2014;8(3):168-174. doi: 10.1177/1938640014557075
[10] Moon D, Jung J. Effect of incorporating short foot exercises in the balance rehabilitation of flat foot: a randomized controlled trial. Healthcare. 2021;9(10):1358. doi: 10.3390/healthcare9101358
[11] Cheng J, Han D, Qu J, et al. Effects of short foot training on foot posture in patients with flatfeet: a systematic review and meta-analysis. Journal of Back and Musculoskeletal Rehabilitation. 2024;37(4):857-872. doi: 10.3233/BMR-230226
[12] Burns J, Crosbie J, Hunt A, Ouvrier R. The effect of pes cavus on foot pain and plantar pressure. Clinical Biomechanics. 2005;20(9):877-882. doi: 10.1016/j.clinbiomech.2005.03.006
[13] Burns J, Crosbie J. Weight bearing ankle dorsiflexion range of motion in idiopathic pes cavus compared to normal and pes planus feet. The Foot. 2005;15(2):91-94. doi: 10.1016/j.foot.2005.03.003
[14] Williams DS 3rd, McClay IS, Hamill J. Arch structure and injury patterns in runners. Clinical Biomechanics. 2001;16(4):341-347. doi: 10.1016/S0268-0033(01)00005-5
[15] Smith TO, Jerman E, Easton V, Bacon H, Armon K, Poland F, Macgregor AJ. Do people with benign joint hypermobility syndrome (BJHS) have reduced joint proprioception? A systematic review and meta-analysis. Rheumatology International. 2013;33(11):2709-2716. doi: 10.1007/s00296-013-2790-4
[16] Kennedy PM, Inglis JT. Distribution and behaviour of glabrous cutaneous receptors in the human foot sole. The Journal of Physiology. 2002;538(3):995-1002. doi: 10.1113/jphysiol.2001.013087
[17] Robbins S, Gouw GJ, McClaran J. Shoe sole thickness and hardness influence balance in older men. Journal of the American Geriatrics Society. 1992;40(11):1089-1094. doi: 10.1111/j.1532-5415.1992.tb01795.x